中文
中文 English
English
- 全国咨询热线
18763018268 15866799466

打造聚甘油酯产业
领航者

总投资1亿元人民币,年产能10000吨

拥有专业化生产技术,建有产品质量控制体系

与国内高校及科研院所紧密合作,拥有专业化技术团队

建立严谨的质控规范,实现原料-生产-产品品质联动

期待新产品新技术合作研发,与客户同进步共发展

实现业务人员对接服务, 完善专业团队结对服务

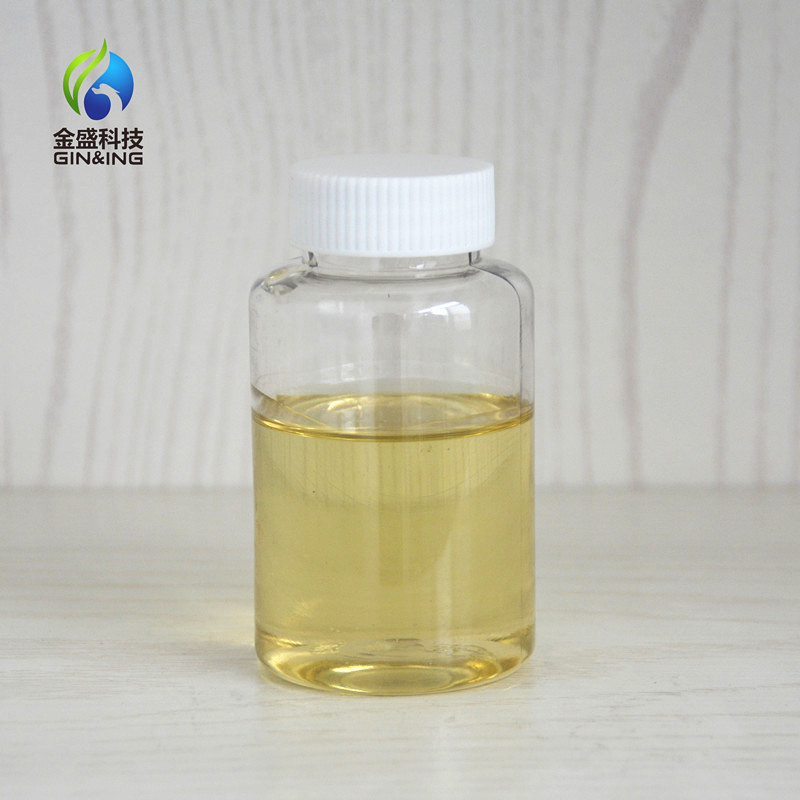
【产品介绍】 产品名称:聚甘油-6辛酸酯 六聚甘油单辛酸酯 英文名称:Polyglycerol -6 caprylate CAS:51033-35-3 外观:黄色油状液体 【产品功效】...
久赢国际登录网址 11286 2023-07-29
【产品介绍】 产品名称:聚甘油-10辛酸酯 十聚甘油单辛酸酯 英文名称:Polyglycerol -10 caprylate CAS:51033-41-1 外观:黄色油状液体 【产品功效】...
久赢国际登录网址 3219 2023-07-29

本品是用植物来源的聚甘油脂肪酸酯,植物油等复配而成的起酥油,不含反式脂肪酸,软硬度,亲水性等可调整。起酥油能使制品分层、膨...
久赢国际登录网址 2695 2023-07-22
肉豆蔻酸酯类乳化剂 肉豆蔻酸(Myristic Acid)是化妆品中广泛使用的一种成分,可作为润肤剂在皮肤上形成保护层,修复、再生和保持其天然...
久赢国际登录网址 823 2023-06-08

产品介绍: 本品是由食品级聚甘油脂肪酸酯,以及食品级其他助剂复合而成的,流动性好,具有良好增溶效果的增溶剂。可替代tween80等部分...
久赢国际登录网址 868 2023-05-17
久赢国际登录网址-点击进入
地址:中国山东滨州高新技术产业开发区
全国咨询热线:18763018268 15866799466
Email:875897441@qq.com
手机:18763018268 15866799466
传真:0531-88021668